Long before testosterone was first identified and synthesised, the role of the testes in male development was understood. For millennia, castration has been used to emasculate men, remove their
vitality, and even produce obedient slaves. Aristotle (384-322 BC) described the effects of castration in both humans and animals in his early biological writings, and research into castration has been carried out right up to the modern day.
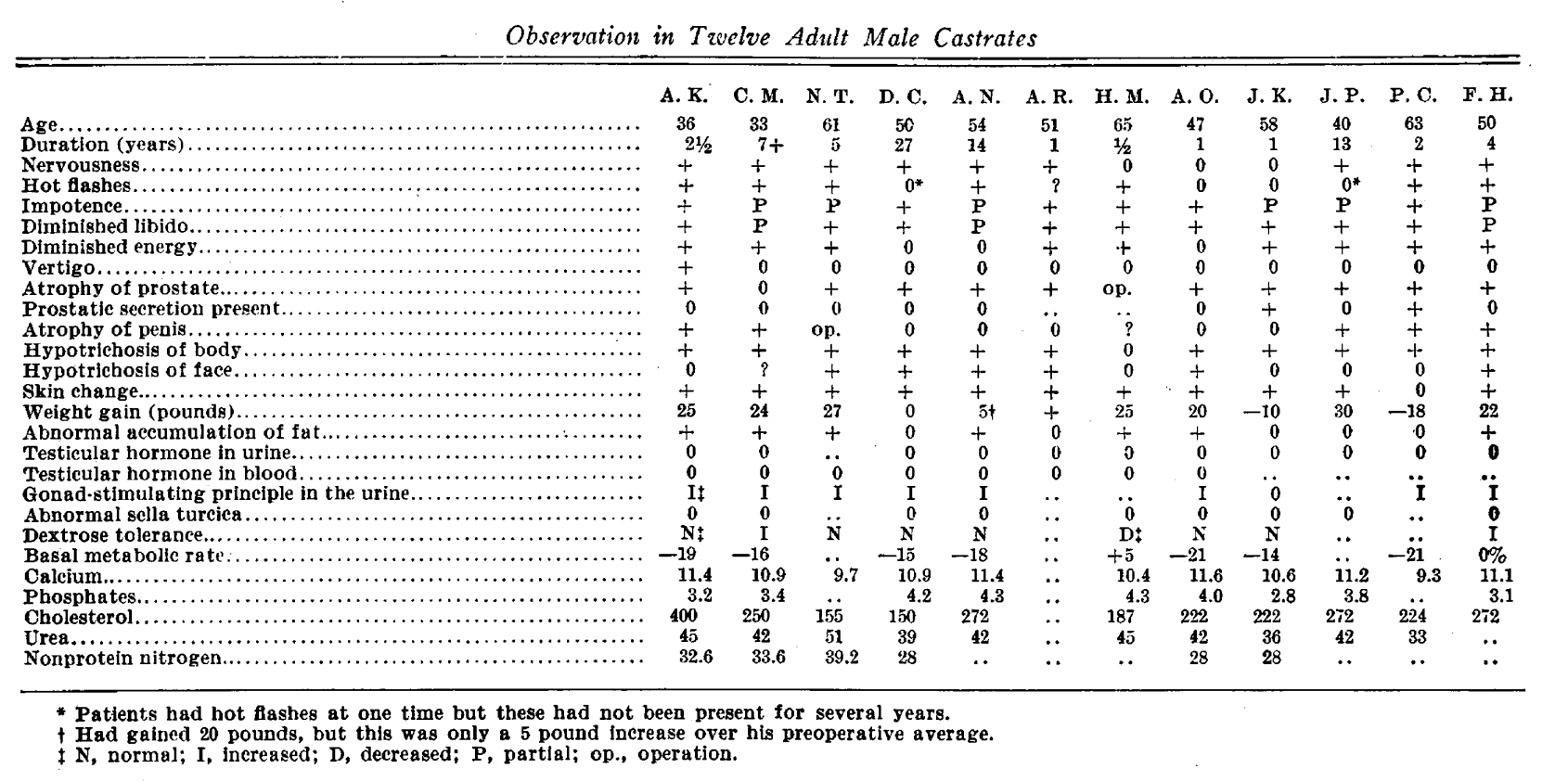
In 1934, the year before testosterone's isolation, the following findings were observed in 12 male castrates, all of which concord with our modern understanding of testosterone (McCullagh et al. 1934).
However, it was in 1935 that testosterone's secrets began to really unfold. Ernst Laqueur (1866–1947) and his group at the University of Amsterdam and at Organon were the first to isolate and name testosterone, having derived just 10mg from 100kg of bull testicles (Butenandt et al. 1935). Since then, we have learned a lot about testosterone, including what makes it increase/decrease, how excesses can harm our health, and how deficits can compromise health, performance, and body composition.
Here are 3 things you may not know about the key hormone of masculinity, testosterone...
(1)Women Have More Testosterone Than Estrogen
While testosterone is indeed a key hormone of masculinity, a little known fact is that women still have more testosterone than estrogen. This doesn't necessarily mean all that much in biology, as concentration is not the sole determinant of biological actions, but it's worth noting nonetheless.
Total Testosterone in young women is generally between 8–60 ng/dL (0.3–2.1 nmol/L), vs 300-1000 ng/dL (10-35 nmol/l) in men. Therefore, sex differences are not just double or triple; we are talking about differences of 10-100x testosterone in men.
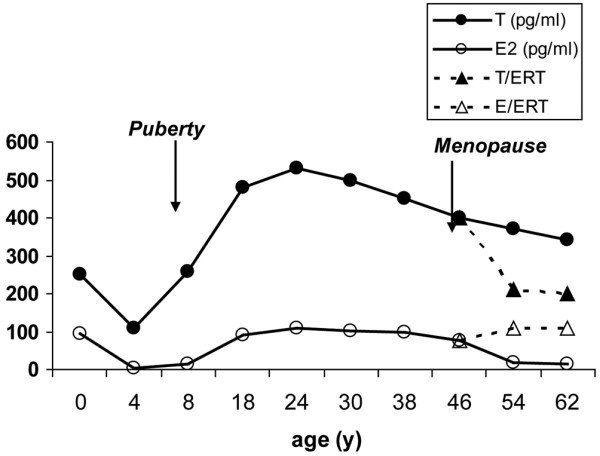
Average estradiol (E2) and testosterone (T) levels across the female lifespan. Y-axis, level in picograms; X-axis, age in years. Dashed lines predict changes
in T and E2 hormone levels resulting from estrogen replacement therapy (ERT) beginning at menopause.
Testosterone plays an important role in women nonetheless. The role of testosterone can be ascertained in women with
polycystic ovarian syndrome (PCOS), where hyperandrogenism is a key biochemical feature. The two dominant biologically active androgens are testosterone & dihydrotestosterone (DHT).
While many of the side effects of hyperandrogenism in
women with PCOS are thought to be undesirable (e.g. Hirsutism, acne, androgenic alopecia), it’s also worth asking if there are advantages to this hyperandrogenic state?
This would seem to be the case. Women with PCOS are over represented in
elite sport (e.g. Olympic athletes), as the hyperandrogenic state seems to support a more muscular physique with stronger bones and a greater VO2max, thus supporting high performance.
Women can also suffer the effects of low testosterone,
including reduced libido, fatigue, weakness, hair loss, and more. This is especially true during menopause, and recent research indicates that testosterone use in postmenopausal women may offset some unwanted effects (Islam et al. 2019).
(2) High AND Low Body Fat Reduce Testosterone
As with many hormonal disruptions, undernourishment tends to reduce testosterone levels. This is unlikely to be surprising, as a lack of energy necessarily leads to energy conservation in the body, and testicular function is one such non-essential energy sink that would not be required in a state of starvation. We see this in cases of female hypothalamic amenorrhoea, relative energy deficiency in sport, diet-induced hypothyroidism, and in this case,
hypotestosteronaemia.
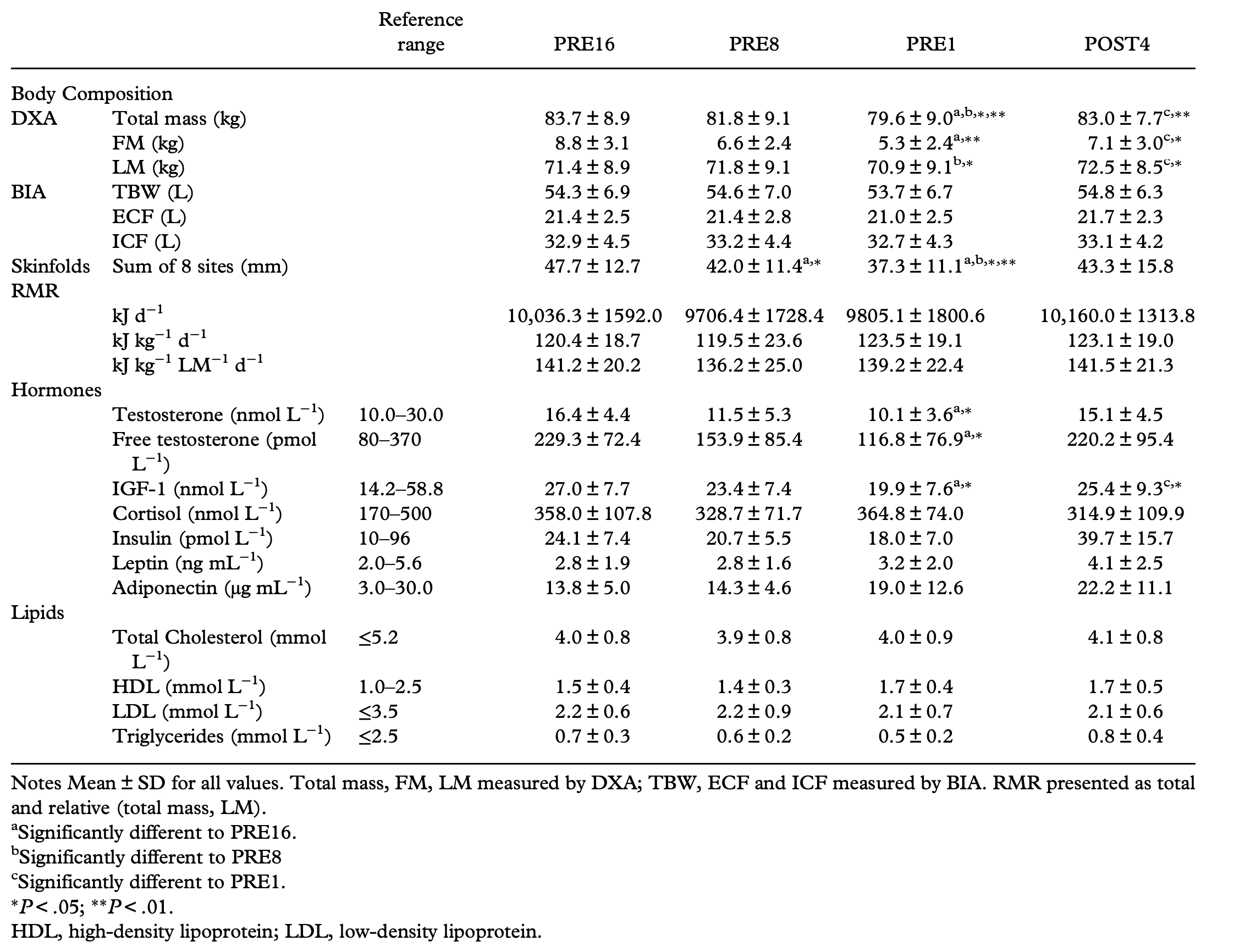
Mitchell et al. (2018) assessed testosterone levels in natural
bodybuilders preparing for competition, and observed large reductions in total and free testosterone from Week 16 pre-competition to Week 1 (16.4 vs. 10.1 nmol/L; 229.3 vs. 116.8 pmol/L). This decline mostly recovered at 4 weeks post-competition, at which point energy intake and body fat had increased once again.
However, it's not quite as simple as "eat more to boost
testosterone". Unfortunately, as we overeat and gain body fat, we can also compromise testosterone levels, as observed in men with obesity. This is no surprise, as we know that aromatase activity in body fat ramps up the conversion of testosterone to estrogen, and obesity-associated metabolic syndrome also drives various endocrine dysfunctions related to insulin resistance, sex-hormone binding globulin, and more.
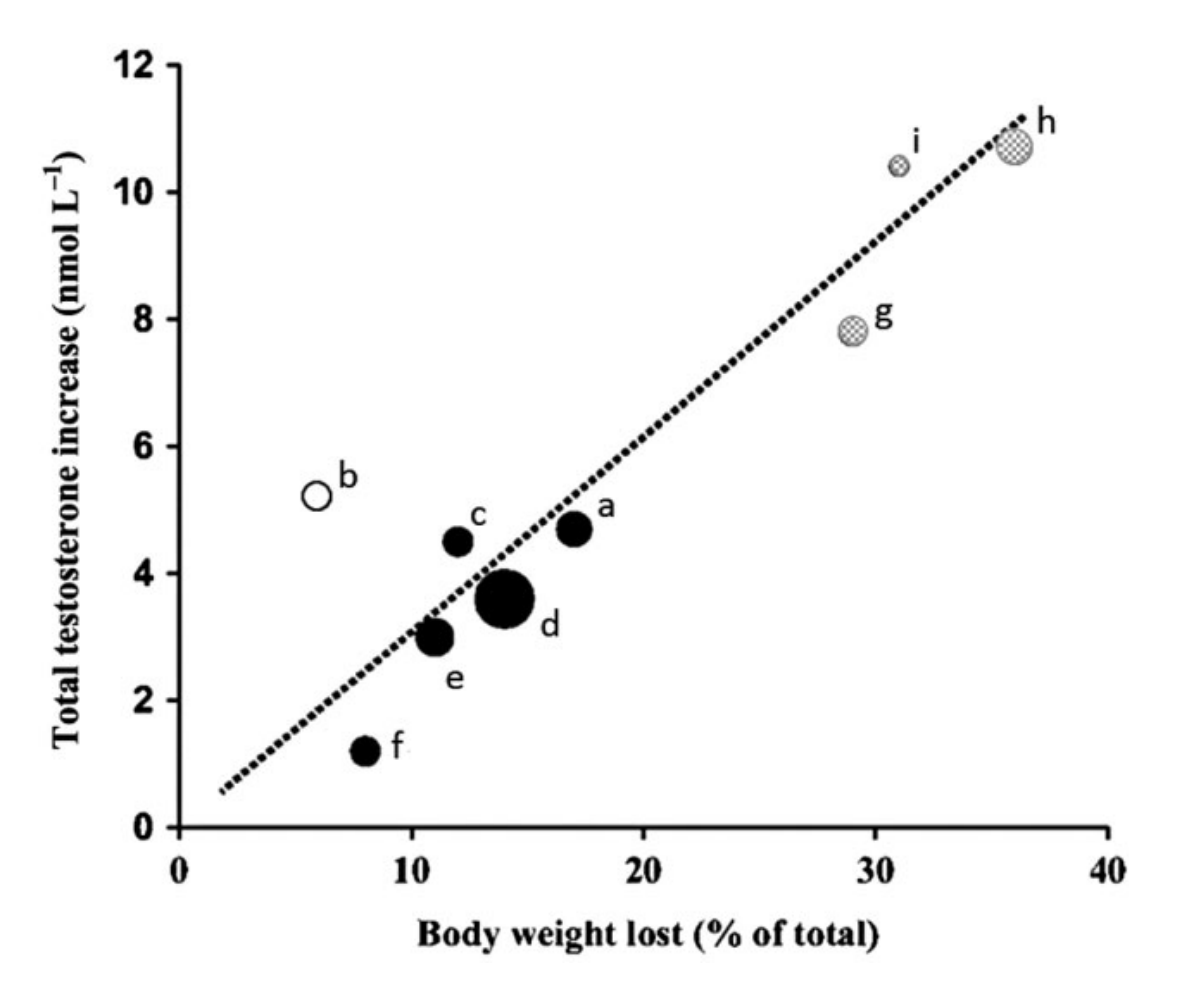
So, does weight loss then lead to increased testosterone? Yes.
Effect of weight loss on
testosterone levels. Each data point refers to an individual study, and the size of the data point is proportional to the size of the study. Figure via Kelly et al. (2015).
The challenging thing in the case of obesity is that there is also a bidirectional relationship here. Obesity reduces testosterone, but testosterone deficiency also promotes obesity and generally
poor body composition. Therefore, the last decade or so has produced increasing interest in testosterone replacement for obese men, as discussed in detail in this paper by Kelly et al. (2015).
(3) Taking Testosterone = Contraception?
With the rise in male-centred health & wellness podcasts, there has been increasing talk of testosterone-replacement therapy (TRT) for men as they enter their 30s and 40s. I have spoken to friends who were considering taking some low dose testosterone, despite the fact that they were currently trying to conceive. Many men seem unaware that testosterone has contraceptive effects, so let's walk through the mechanisms at play.
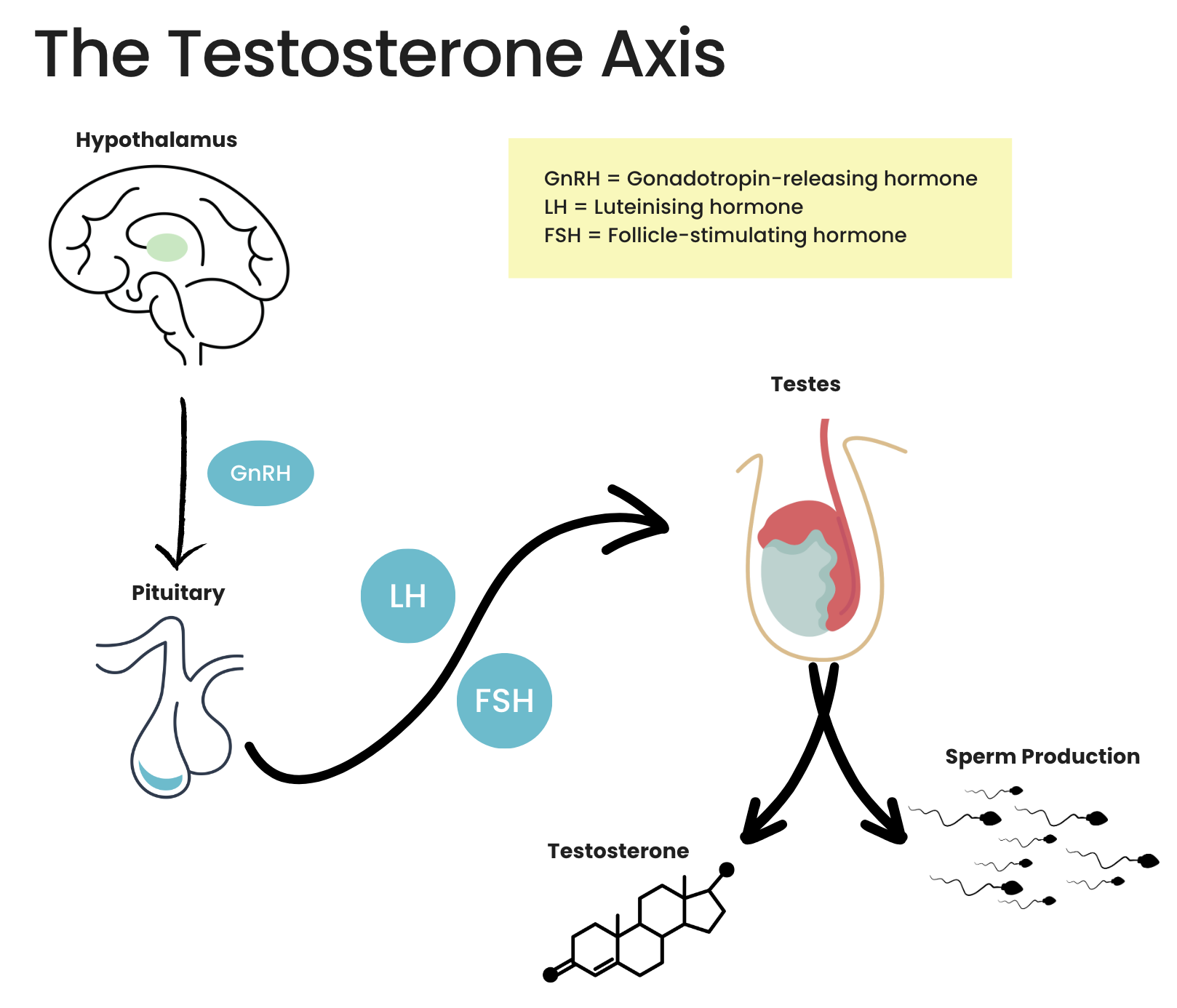
Exogenous testosterone use increases circulating testosterone in the body. This signals that "we have enough testosterone", causing the testicles to reduce testosterone production, sperm count, and thus testicular shrinkage is observed. Let's take a look at the
normal hormonal axis (hypothalamic-pituitary-gonadal axis) at play here...
These are the normal events. There are more steps not discussed here, including the roles of the Sertoli and Leydig cells, along with various other hormones, but this will suffice for this conversation.
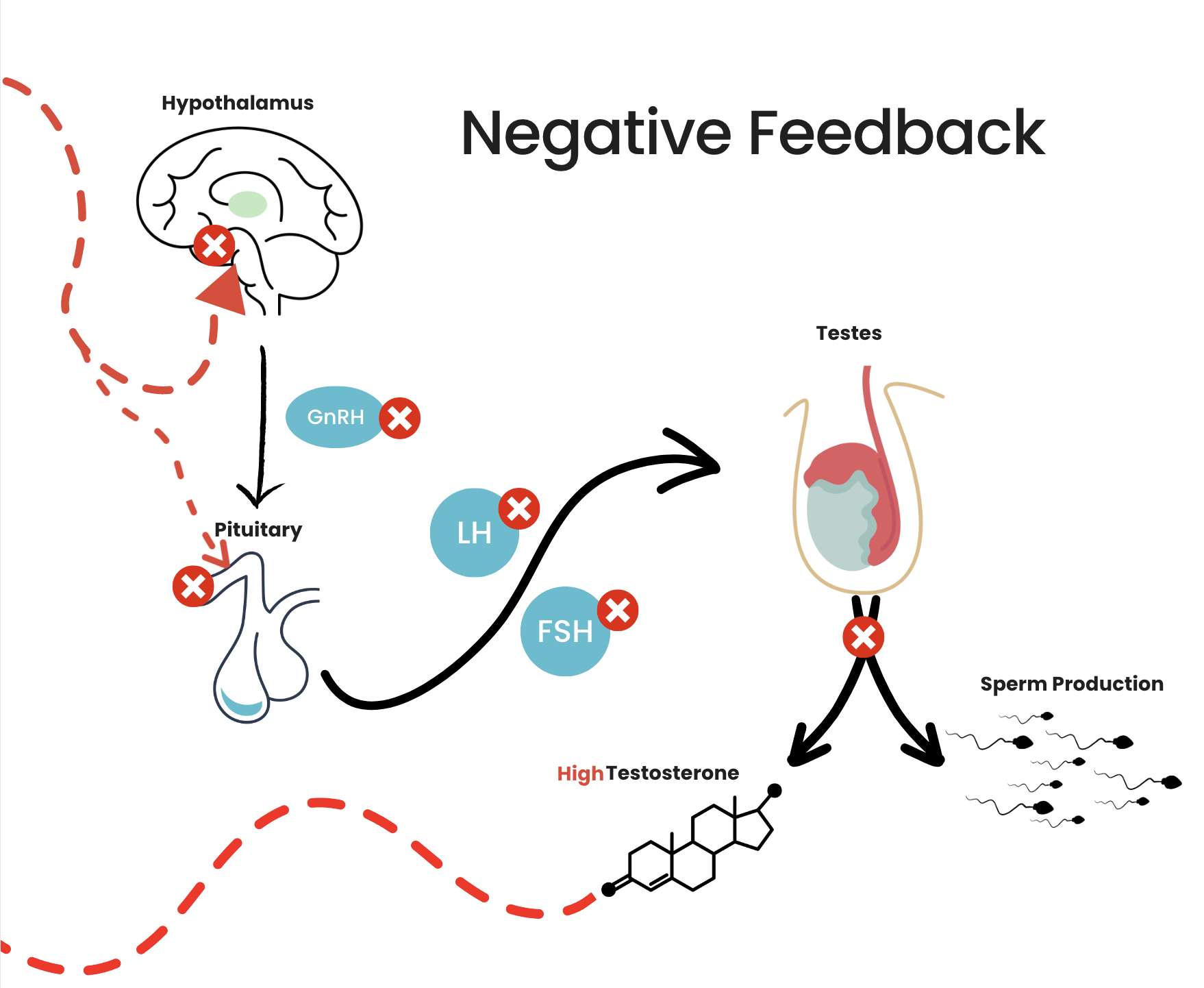
Here is what happens when we introduce exogenous testosterone that drives up serum testosterone...
When testosterone levels are high, this feeds back to the hypothalamus
& pituitary to tell them that we don't need to keep making more, reducing testicular output.
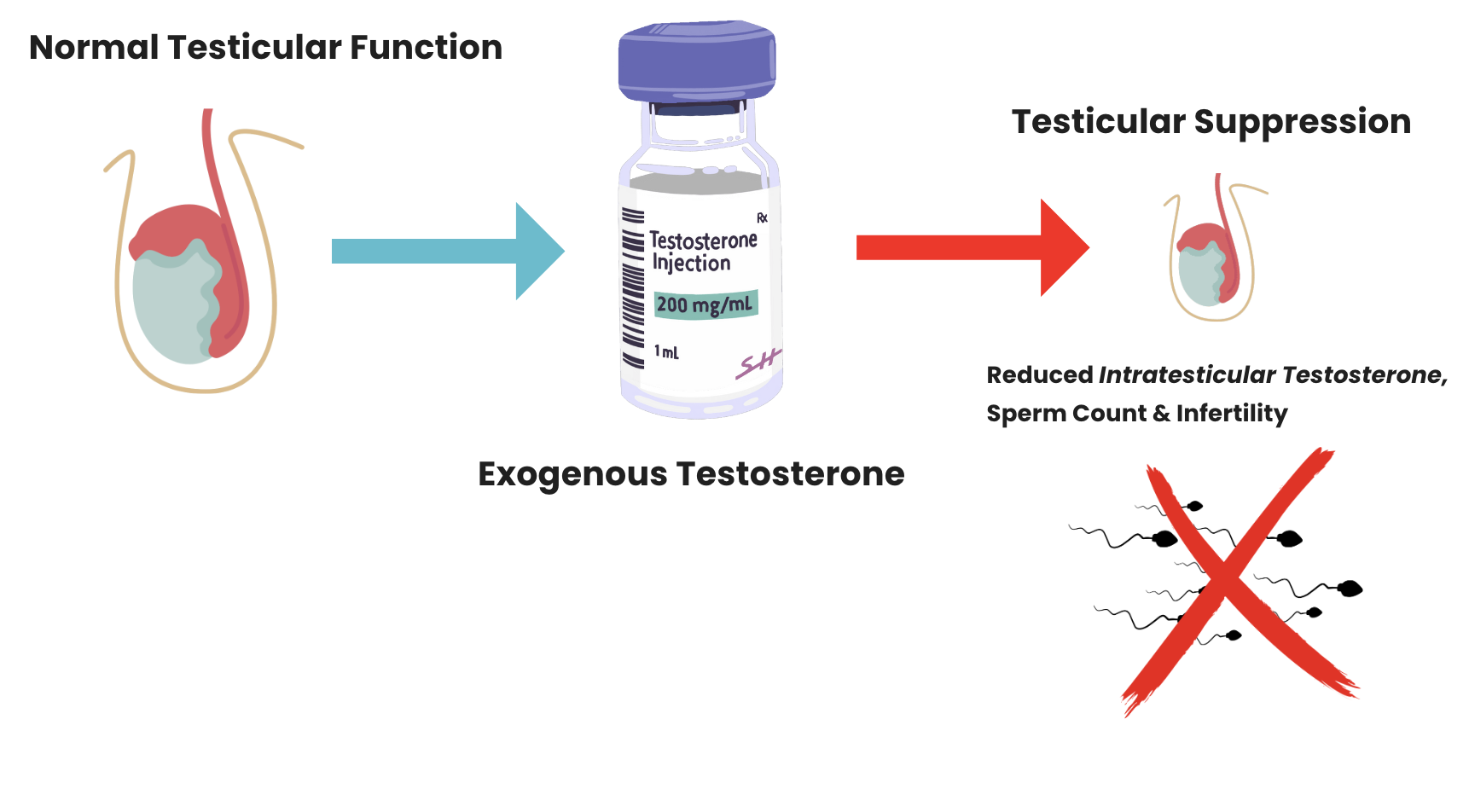
Intratesticular testosterone and gonadotropin signalling, not serum testosterone, are most important for the preservation of fertility. The
testicles are normally a testosterone-rich environment with 100x the testosterone of serum, and it's in this environment that spermatogenesis thrives.
The good news is that, while these effects occur short term, recovery can often take place, albeit incomplete in some cases. In this study, 271 men
received 200mg Testosterone Enanthate weekly for 6 months. At 6 months, 65% were azoospermic, meaning they had zero sperm in their ejaculate. During the recovery period, 85% of men achieved sperm density >20 million/mL at median ~3.7 months, but just 46% recovered baseline sperm density.
In summary, one should take great care in knowing exactly what the repercussions of TRT and/or anabolic steroid use are prior to jumping in. There are lots of guys out there using testosterone that are totally unaware of the repercussions for their fertility.
References
Butenandt A, Hanisch G. Über Testosteron . Umwandlung des Dehydroandrosterons in Androstendiol und Testosteron; ein Weg zur Darstellung des Testosterons aus Cholesterin. Hoppe-Seyler’s Zeitschrift für Physiologie und Chemie 1935 237 89–97.
Islam, R. M., Bell, R. J., Green, S., Page, M. J., & Davis, S. R. (2019). Safety and efficacy of testosterone for women: a systematic review and meta-analysis of randomised controlled trial data. The lancet. Diabetes & endocrinology, 7(10),
754–766. https://doi.org/10.1016/S2213-8587(19)30189-5
Kelly, D. M., & Jones, T. H.
(2015). Testosterone and obesity. Obesity Reviews, 16(7), 581–606. doi:10.1111/obr.12282
McCullagh EP, Renshaw JF. The Effects of Castration in the Adult Male. JAMA. 1934;103(15):1140–1143. doi:10.1001/jama.1934.02750410030006
Mitchell, L., Slater, G., Hackett, D., Johnson, N., & O’connor, H. (2018). Physiological implications of preparing for a natural male bodybuilding competition. European Journal of Sport Science, 18(5), 619–629.
doi:10.1080/17461391.2018.1444
Contraceptive efficacy of testosterone-induced azoospermia in normal men. World Health Organization Task Force on methods for the regulation of male fertility. Lancet 1990;336:955-9.
Before I go, do note that we have coaching spaces available currently. If you'd like to work with the Triage Team toward
your goals, we are currently taking on clients. Simply pop your details in here.
Supplementation can enhance your workout performance, thus contributing to better strength, endurance, and exercise motivation. Here are the peri-workout supplements that actually
work!